🏅 Scientific Research Poster Winner
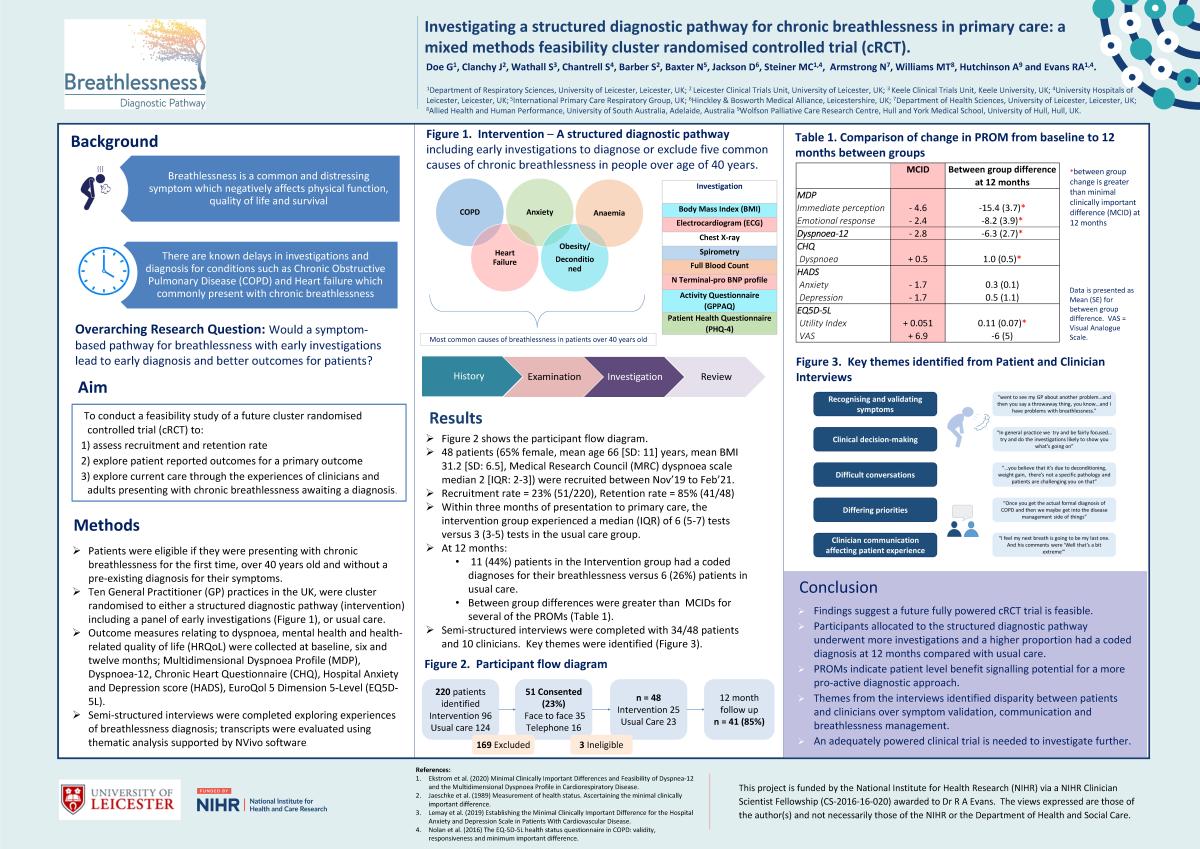
Investigating a structured diagnostic pathway for chronic breathlessness in primary care: a mixed methods feasibility cluster randomised controlled trial (cRCT). (ID 389)
University of Leicester
Abstract
Aim
To assess feasibility of a cRCT investigating a structured diagnostic pathway versus usual care for adults with chronic breathlessness in primary care.
Methods
Ten GP practices were cluster randomised to a structured diagnostic pathway including a panel of early investigations (Intervention group [IG]) or Usual care (UC). Eligible patients were recruited opportunistically: ≥40 years old, first presentation of chronic breathlessness, no prior diagnosis for breathlessness. Feasibility outcomes included recruitment and retention rate. Number of investigations and coded diagnoses were recorded from healthcare records. Patient reported outcome measures (PROMs) for breathlessness, mental health and health-related quality of life were collected at baseline, six and 12 months. Semi-structured interviews were completed exploring experiences of breathlessness diagnosis; transcripts were evaluated using thematic analysis supported by NVivo software.
Results
48 /220 (22%) patients were recruited between November 2019 and February 2021: 65% female, mean (SD) age 66(11) years, BMI 31.2(6.5), median (IQR) MRC dyspnoea scale 2(2-3). 41/48 (85%) participants returned PROMs. The IG had a median (IQR) of 8(7-9) tests compared with 5(3-6) tests in UC within three months. At 12 months, 11/45 (44%) patients in the IG had a coded diagnoses for their breathlessness versus 6/23 (26%) patients in UC. Table 1 presents PROMs comparisons between groups.
Semi-structured interviews were completed with 34/48 patients and 10 clinicians (mean [SD] 17 [6.3] years’ experience, 5 [50%] female, 7 [70%] White British). Key themes were identified (Figure 1).
Conclusion
Recruitment and retention rate indicate a cRCT investigating a structured diagnostic pathway in primary care is feasible. The IG underwent more investigations and more patients had a recorded coded diagnosis at 12 months compared with UC. PROMs indicate potential patient level benefit. Themes from the interviews identified disparity between symptom validation, communication and breathlessness management. An adequately powered clinical trial is needed to investigate further.
Funding: This work was funded by a NIHR Clinician Scientist Fellowship (CS-2016-16-020) awarded to Dr Rachael A Evans.
Conflicts of interest: None.