Implementation of a Computer Guided Consultation (intelligent clinical decision support system software) for COPD patients in NHS Bedfordshire: evaluation of clinical and health economic benefits (ID 296)
Liverpool University Hospitals NHS Foundation Trust
Abstract
Implementation of a Computer Guided Consultation (intelligent clinical decision support system software) for COPD patients in NHS Bedfordshire: evaluation of clinical and health economic benefits
Biswajit Chakrabarti1&2, Mike Pearson1&2, Eddie McKnight2, Lisa Davies1&2, Phil England2, Louise Reed2, Kim Sergeant2, Robert Angus1&2
1. University Hospital Aintree, Liverpool University Hospitals NHS Foundation Trust
2. Lunghealth Ltd
Introduction: COPD is a common source of morbidity, mortality and healthcare utilisation within primary care. We describe the impact of implementing the LungHealth COPD Clinical Guided Consultation (CGC) in the NHS Bedfordshire CCG locality focusing on key clinical and health economic benefits.
Methodology: The CGC is an intelligent clinical decision support system enabling the user to confirm the correct diagnosis of COPD with multiple algorithms integrating history, physical signs and interpretation of spirometry subsequently staging COPD according to established guidelines. Once reaching the correct diagnosis, the CGC prompts guideline based management where appropriate including pharmacological therapy, smoking cessation, oxygen clinic assessment and identifying patients suitable for secondary care referral.
Result: 847 patients on the COPD register in NHS Bedfordshire CCG were reviewed across 17 practices from March 2019-March 2020 comprising 19% of the COPD population. Following CGC review, 18% (146/847) were found not to have the diagnosis of COPD (McNemar’s test; p<0.001). In those diagnosed with COPD, those with adequate inhaler technique and a written management plan increased from 68% to 94.8% and 44.4% to 92.1% respectively from pre to post CGC review (McNemar’s test; p<0.001). 12% were referred for Smoking Cessation and 8.1% of subjects were referred for pulmonary rehabilitation. One or more COPD medication was discontinued in 43% (382/847) whilst new COPD medication was commenced in 29% (244/847). Implementation of the CGC is believed to have delivered a net potential saving of around £200,000 resulting from discontinuation of medications/ further follow up visits in those misdiagnosed, from reconciliation of existing medications to meet established guidelines and in optimising existing medications to reduce healthcare utilisation.
Conclusion: The implementation of a clinical guided consultation within primary care enables COPD patients to be diagnosed correctly, drives appropriate guideline level management resulting in clinical and health economic benefit and addresses health inequality.
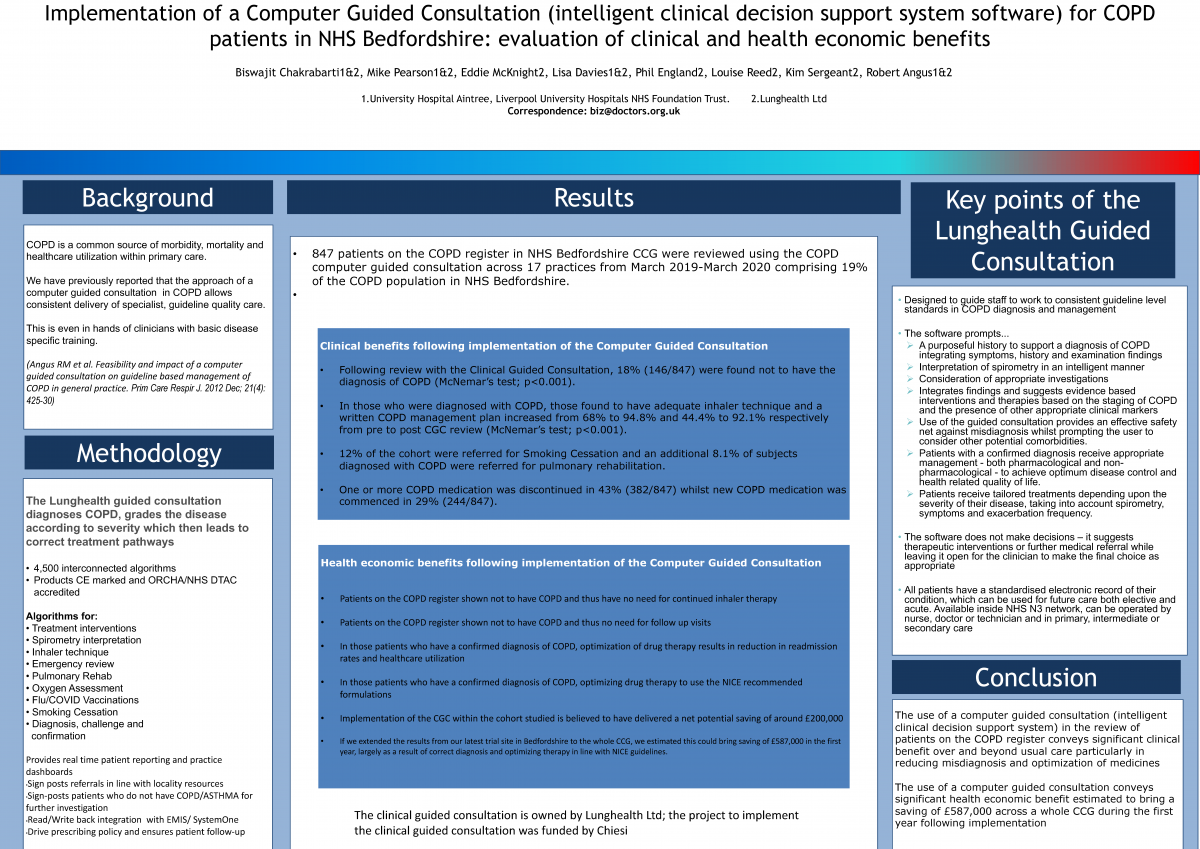
Funding: The project was funded by Chiesi
Conflicts of interest: The CGC is owned by LungHealth. Dr Chakrabarti, Dr Angus, Dr Davies, Professor Pearson and Mr McKnight are directors of Lunghealth.