Withdrawal of inhaled corticosteroids in patients with COPD: a descriptive study using primary care electronic records (ID 390)
University of Oxford
Abstract
Aim
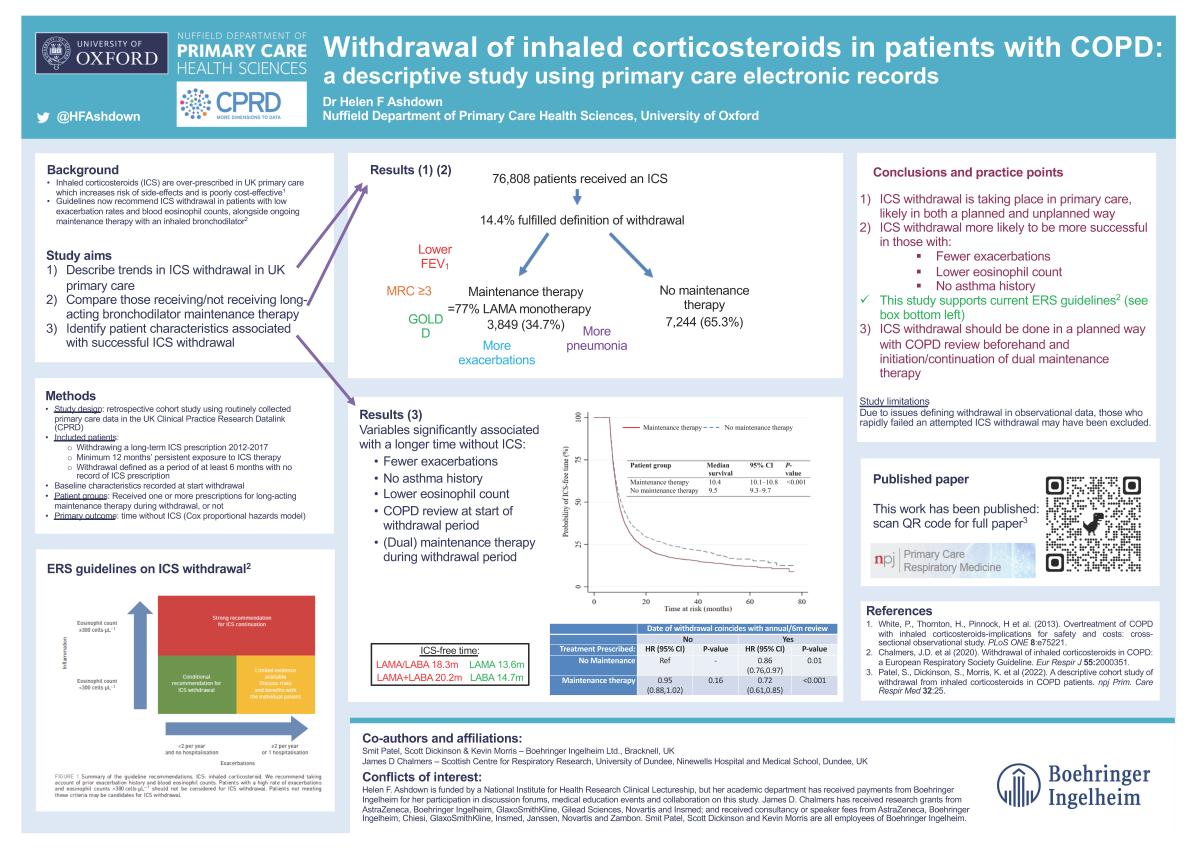
Inhaled corticosteroids (ICS) are over-prescribed in UK primary care, which increases risk of side-effects and is poorly cost-effective. Guidelines now recommend ICS withdrawal in patients with low exacerbation rates and blood eosinophil counts, alongside ongoing maintenance therapy with an inhaled bronchodilator. We aimed to describe trends in ICS withdrawal and outcomes for patients receiving or not receiving maintenance bronchodilators, and to identify patient characteristics associated with successful ICS withdrawal.
Method
This was a retrospective cohort study using routinely collected primary care data in the UK Clinical Practice Research Datalink (CPRD). Included patients had a coded diagnosis of COPD ≥35 years and were withdrawing a long-term ICS prescription between 2012-2017: defined as a minimum historical period of 12 months’ persistent exposure to ICS followed by at least 6 months with no record of ICS prescription. Baseline characteristics were recorded at the start of withdrawal, and whether patients received any prescriptions for maintenance therapy during withdrawal. Primary outcome was the time without ICS, with hazard ratios calculated for baseline variables using a Cox proportional hazards model.
Results
76,808 patients received an ICS, of whom 11,093 (14.4%) fulfilled the definition of withdrawal. 3,849 (34.7%) received maintenance therapy and 7,244 (65.3%) did not. Those receiving maintenance therapy had more severe disease at withdrawal. Median ICS-free time after withdrawal was longer in those receiving maintenance therapy than those who did not (10.4 months (95% CI 10.1-10.8) vs. 9.5 months (95% CI 9.3-9.7), p<0.001), and where the date of withdrawal coincided with a COPD annual review (combined HR for maintenance therapy and annual review 0.72 (95% CI 0.61-0.85, p<0.001).
Conclusion
ICS withdrawal success can be enhanced by COPD reviews and use of maintenance therapy alongside. Limitations of the study include potentially excluding those who may have rapidly failed an attempted withdrawal.
Funding: Boehringer Ingelheim staff conducted this research as part of their employment but received no additional funding. External researchers (Helen Ashdown and James Chalmers) received payments from Boehringer Ingelheim for their time in collaborating in this work.
Conflicts of interest: Helen F. Ashdown is funded by a National Institute for Health Research Clinical Lectureship, but her academic department has received payments from Boehringer Ingelheim for her participation in discussion forums, medical education events and collaboration on this study.
James D. Chalmers has received research grants from AstraZeneca, Boehringer Ingelheim, GlaxoSmithKline, Gilead Sciences, Novartis and Insmed; and received consultancy or speaker fees from AstraZeneca, Boehringer Ingelheim, Chiesi, GlaxoSmithKline, Insmed, Janssen, Novartis and Zambon.
Smit Patel, Scott Dickinson and Kevin Morris are all employees of Boehringer Ingelheim.
The conference has been instigated and organised by PCRS. We are grateful to sponsors and exhibitors who have contributed funding towards this event in return for exhibition space. Neither sponsors or exhibitors have had any input into the agenda or the selection of speakers with the exception of any sponsored satellite symposia which are clearly indicated. View the full list of sponsors.