Blog series – Asthma outcomes: Psychology perspective | Dr Alistair JA Duff
Dr Alistair JA Duff is a Consultant Clinical Psychologist and is Honorary Clinical Associate Professor at the University of Leeds. He leads us through some of the psychological issues which contribute to the UK’s asthma outcomes trailing behind other nations. |
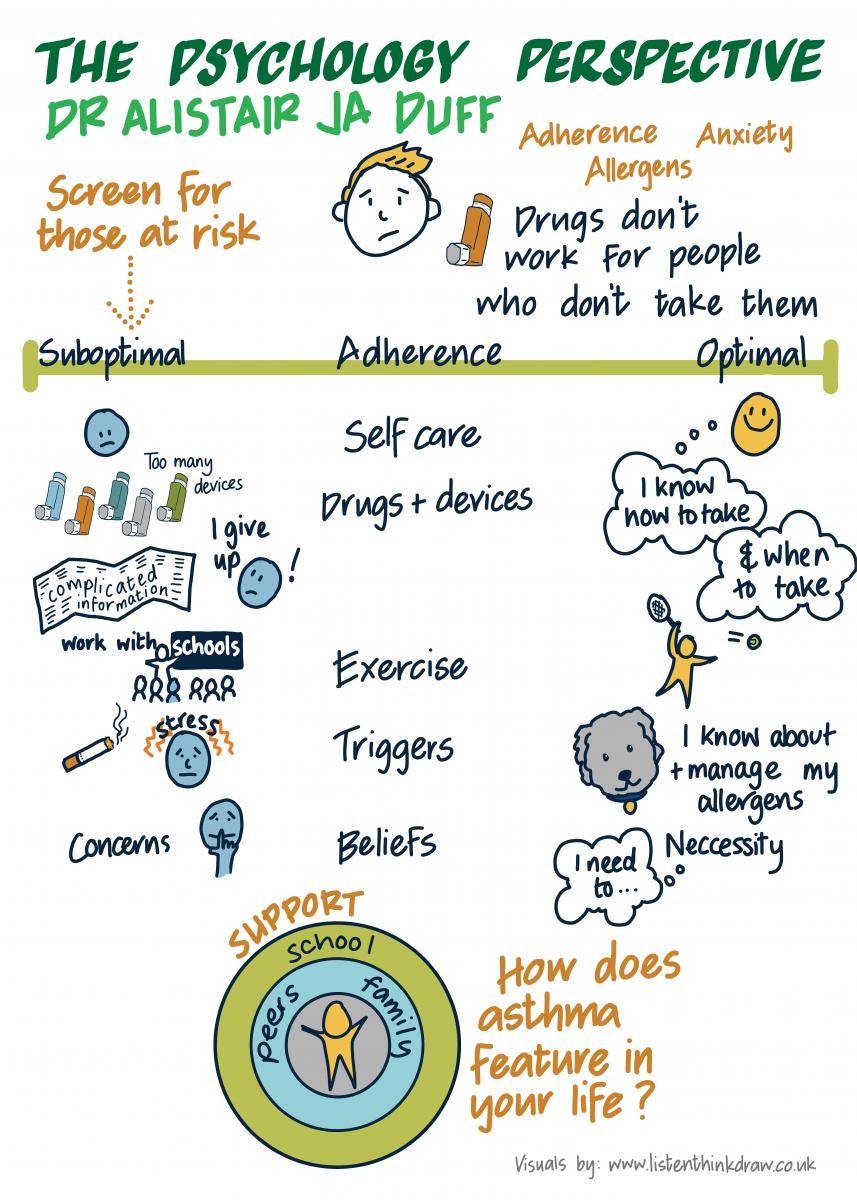
I’ve been working in asthma clinics for a while now and I’ve been struck by how often the problems with achieving good asthma control are rooted in emotional and/or behavioural problems, rather than medical ones, difficulties with accepting asthma, anxiety and adherence being most common.
The simple fact is that drugs don’t work in people who don’t take them. Although that may seem trite, it is sometimes the very simple things that we need to focus on to help people achieve good asthma control; listening and understanding the impact on their lives, helping them automate daily care, constantly reviewing options to reduce the burden of care (new devices, new drugs, new routines).
I often talk about the difference between optimal adherence and sub-optimal adherence, rather than poor adherence or non-adherence. It’s rare that somebody doesn’t take absolutely anything, and it’s equally rare that they take it 100% correctly. We’re looking at the margins of what we would consider clinically optimal and sub-optimal which gives us scope to work with people in different ways.
Optimal adherence will depend on optimal control. How do we improve optimal control? We can start with encouraging self-care behaviours and minimizing exposure to triggers
Self-care behaviours
We’re trying to get people to adopt good self-care behaviours. These can include a range of things that people have to do when they have any chronic condition.
- Adherence - Learning how and when to take their medicines, as well as what to take
- Device technique - In asthma I think we have got a problem with device techniques. There are very many different drug-device combinations, all with different instructions. So even the simplest - ‘take two puffs twice a day’ recommendation in clinic - can actually be very complicated
- Exercise – especially with young people, encourage kids to exercise in a way that builds their confidence. That involves working with the school system and parents as well as potentially involving physios in their own clinics.
Minimising exposure to known triggers
We know about smoke, we know about stress in some ways, but we know a lot less about how people expose themselves to sensitivities and allergies.
When you add up all the self-care behaviours we require of patients and families, we are asking a lot in terms of them living their lives with a chronic illness. Asthma is not a simple regimen for people to adapt to, accept and therefore adhere to optimally.
Factors which reduce adherence
So, what are the factors that I would look at when considering a young person who is not adhering optimally? It’s a conflation of factors that are individual, systemic and relating to treatment.
- Individual factors will depend on the age, stage and health beliefs that children and young people (CYP) and their families have about asthma and about its treatments. We always start with the intersection of the age of the child with their psychodevelopmental stage and then consider what role asthma plays in their lives? Does it make them feel more visible at school? Does it make them feel more different at school? What beliefs do they have, right or wrong about inhaled corticosteroids or allergies or wheeze or inflammation? It is important to help individuals (patients and parents) psychologically accept asthma as part of their lives; to stop struggling with it as if they were trying and rid themselves of it. It’s like trying to hold a beach ball underwater. At some stage they will tire and the ball will surface, perhaps when they least want it to. And so the alternative is to consider living their lives differently with asthma and its treatment, and to accept it. This is pivotal in making a successful emotional adaptation to asthma.
- Systemic environments:
- Family: family support, ability to communicate about adherence
- School: kids just see asthma as a barrier and don’t engage in certain activities
- Peer groups: perhaps the most important group for CYP in terms of support and anxiety. There is an emerging view that CYP who have asthma are bullied at school more than their peers. This can add to the stigma of having asthma, which in turn leads young people to want to hide their asthma or it’s treatment
- Treatment: treatments that have little immediate effect and take time which are believed to be intrusive are very unlikely to be taken in any optimal way. ICS fit that bill. I still use the framework of necessities and concerns, which suggests that if you have many more concerns than you have necessity beliefs, you’re very unlikely to take your medicines. This is a simple but very effective model when you are in clinic, trying to explain theory and understanding to people you are trying to help.