Blog series – Asthma outcomes: Research perspective | Professor Hilary Pinnock
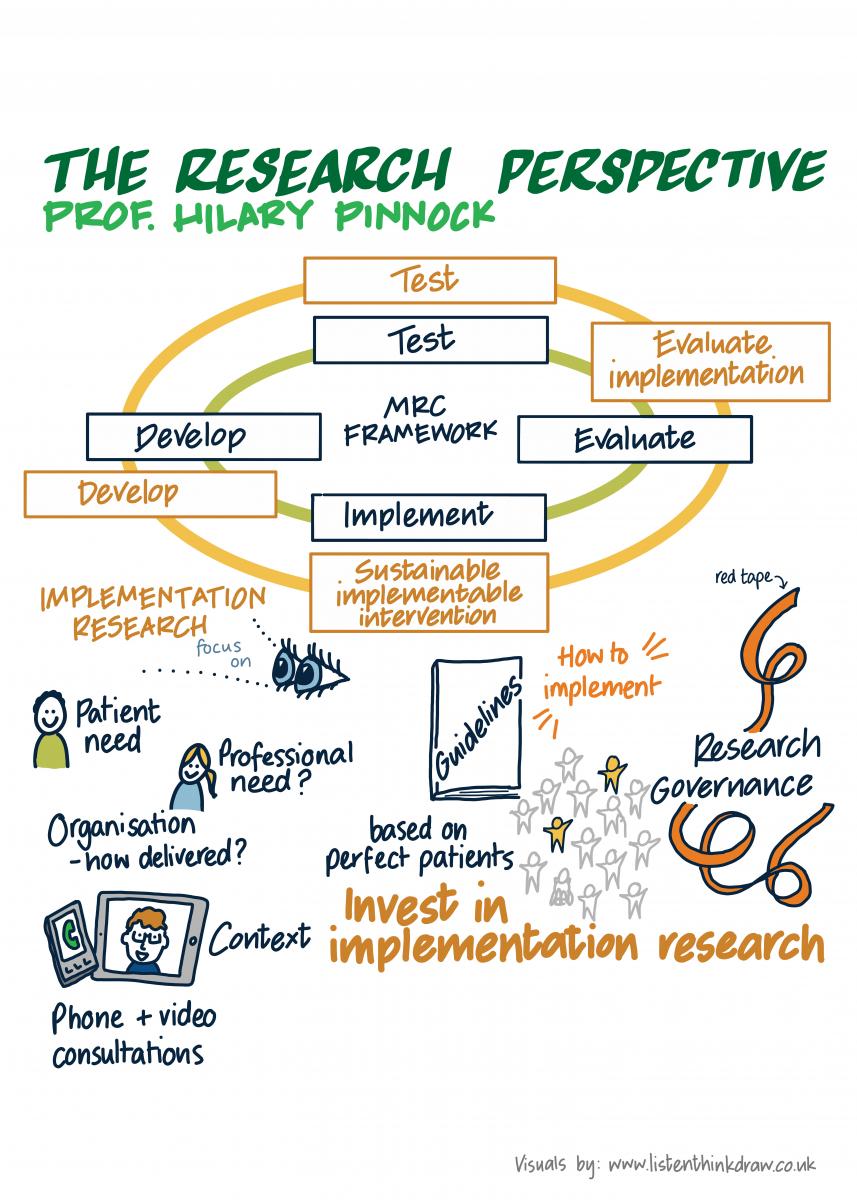
Professor Hilary Pinnock is Professor of Primary Care Respiratory Medicine at the University of Edinburgh and Lead on the Optimising Management of Asthma Attacks theme within the Asthma UK Centre for Applied Research. She takes us through the difficulties in getting research into practice. |
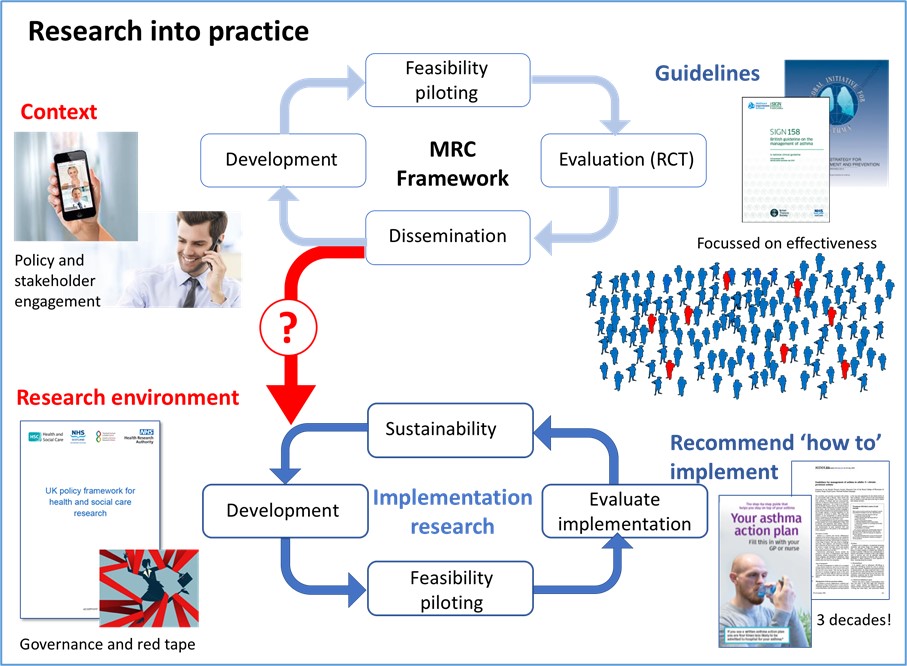
Researchers reading this will recognise the Medical Research Council framework for developing and evaluating complex interventions. The steps are clearly laid out. Develop the intervention; test its feasibility and acceptability; evaluate it in a randomised control trial (RCT); and then (if it proves to be effective) disseminate the findings. Having completed these steps over several years, it is easy to naively think that every practice and clinician in the country will learn from the research findings and implement the intervention in their practice.
Unfortunately, it just doesn’t work like that. There are many reasons for this.
Evidence and guideline recommendations are based on RCT evidence
Most RCTs are do not reflect the real world. RCTs typically recruit ‘ideal’ patients: excluding the elderly, the pregnant, those who don’t adhere to their medications optimally, those who can’t use inhalers and anyone with co-existing illnesses. The result is that only 5-10% of the patients we see in general practice are eligible for most of the RCTs on which evidence-based guidelines are based. In addition, the RCTs designed to test if an intervention is effective will fund the necessary resources and staff to deliver the intervention with high fidelity under ideal circumstances. This is not the real world we live in.
What we need is a second, implementation cycle to develop strategies to implement effective interventions into routine care, testing feasibility and acceptability, and evaluating the implementation strategy whilst exploring sustainability. This is implementation research. Research that defines the patient, professional and organisational practicalities of how an effective intervention can be implemented.
Context is key
Anyone working in implementation research will agree about the crucial importance of context. Here is an example.
Some 15 years ago, I published a paper that showed that if you provided people with asthma with the option of a telephone review instead of having to attend their practice, more people had a review – and their asthma control was no different to the face-to-face group. This all happened at the time that the Quality and Outcomes Framework (QoF) was being introduced which rewarded practices for regularly reviewing their asthma patients. Despite the evidence, telephone reviews were not counted for QoF and effectively banned.
In March 2020, coronavirus hit and overnight we converted all our consultations to remote telephone or video consultations. Bans were lifted, and telephone reviews promoted as the way to provide on-going care in the context of social distancing.
The evidence hadn’t changed – but the context has...
Red tape
Research governance is designed for drug trials, or RCTs of new technologies, not studies designed to test the implementation of an evidence-based – and often guideline-recommended - intervention. As a result, we are constantly completing forms with questions that are ‘not applicable’ to research that is developing and evaluating an implementation strategy.
Getting research into practice
Guidelines could help. Most guidelines stop at recommending the evidence-based intervention. For example ‘Everyone with asthma should be supported to self-manage their condition’ is a recommendation in all national and international guidelines, but they rarely address how this can be achieved in routine clinical practice. The British Thoracic Society/Scottish Intercollegiate Guideline Network British asthma guideline explicitly looked at the ‘how to’ question. That meant searching for implementation research evidence which was reported in a section on how to implement supported self-management in practice. ‘How to’ sections should be central to guideline development.
The UK is a world leader in health service research. We generate the evidence but we need to invest time, money and resources into implementation research such that effective interventions are facilitated into practice.